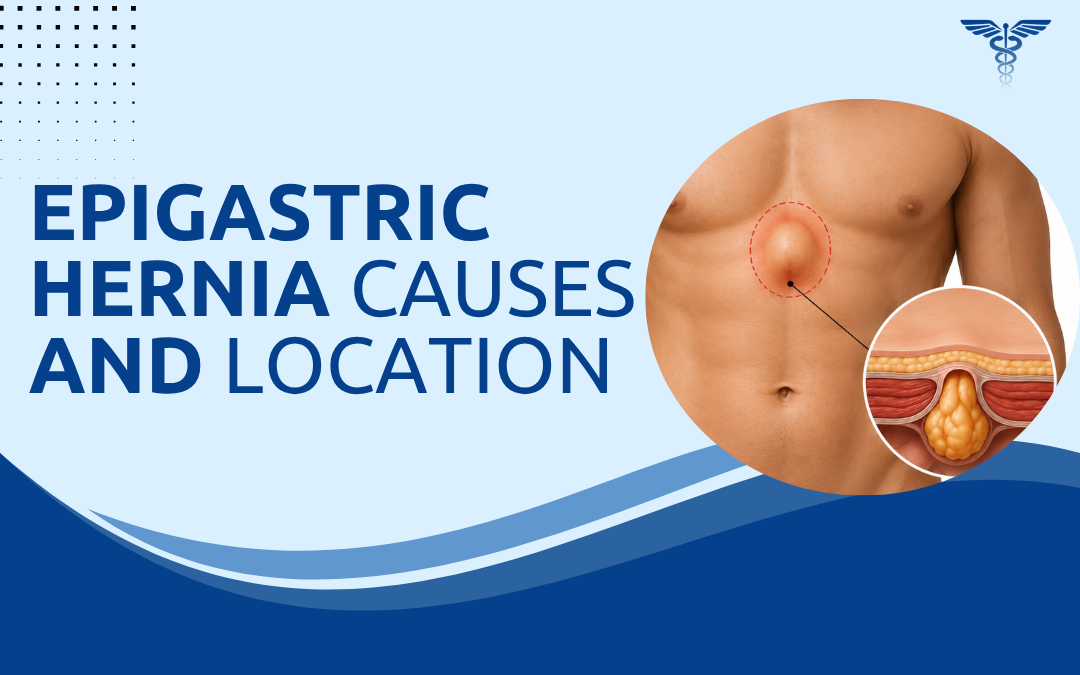
An epigastric hernia is a protrusion of preperitoneal fat through a weakness in the linea alba, the fibrous midline band between the navel and breastbone. The defect is usually small and tight. Most contain fat, not bowel. That tight defect is what generates pain disproportionate to the size of the hernia, which is why patients spend months attributing upper abdominal discomfort to gastritis before the midline is examined.
According to Dr. Rajeev Premnath, a trusted Hernia Specialist in Bangalore, Epigastric hernias get missed because they’re small and the pain gets attributed to gastritis or acid reflux. Patients spend months on antacids before someone examines the midline properly and finds the defect.
What Exactly Is an Epigastric Hernia and Why Does It Form?
The linea alba looks solid on imaging. Under sustained pressure it isn’t, and the defects that form there are small, painful, and consistently missed on superficial examination.
- Location: Strictly midline, between the xiphoid process and the umbilicus. Multiple small defects can coexist in the same patient along the linea alba. The upper third of that space is where the vast majority sit.
- What protrudes: Preperitoneal fat in most cases, not bowel. The defect is tight enough that the fat gets trapped, loses blood supply, and generates localised pain. That’s what brings patients in, not a visible lump.
- Why it forms: Obesity, heavy lifting, chronic cough, multiple pregnancies. All raise intra-abdominal pressure repeatedly over time. Men’s linea alba is anatomically narrower than women’s, which concentrates that pressure into a smaller area and explains the higher incidence in men.
- Symptoms: Firm tender lump in the upper midline, worse after eating or exertion, sometimes disappears lying flat. The pain often gets called indigestion for months. It isn’t.
A tight defect can incarcerate and cause acute pain without warning. A clinical assessment for hernia surgery is needed when the lump or pain pattern fits.
How Is an Epigastric Hernia Diagnosed and Treated?
Diagnosis is clinical in the majority of epigastric hernia presentations. What determines the next step is defect size, symptom burden, and the trajectory of the hernia over time.
- Diagnosis: Patient raises their head from lying flat, linea alba tenses, small defects become palpable that weren’t obvious at rest. Ultrasound confirms size and content. CT when examination is inconclusive or multiple defects are suspected along the midline.
- Watchful waiting: Small asymptomatic hernias with fat content only and no enlargement trend can be monitored. The incarceration risk is low. Low isn’t zero. Follow-up is required, not indefinite deferral.
- Surgical repair: Symptomatic hernias, enlarging defects, and incarcerated presentations need repair. Laparoscopic mesh repair for defects over 1cm. Mesh reduces recurrence significantly at any size compared to primary suture closure alone.
- Recovery: Day-care in most cases. Desk work within one week. Heavy lifting restricted four to six weeks while mesh integrates into the abdominal wall. Recovery matches standard laparoscopic hernia repair closely.
Epigastric hernias don’t close on their own. Our previous blog on epigastric hernia covers how it differs from umbilical hernia in anatomy, presentation, and surgical management.
Why Choose Dr. Rajeev Premnath?
Dr. Rajeev Premnath completed fellowship training in laparoscopy from IRCAD France and SILS certification from NUH Singapore, and holds MBBS, MS (Gen Surg.), FRCS (Glasg.), FEBS, FICS, FACS, FIAGES, FMAS. He has been managing epigastric, umbilical, inguinal, and incisional hernias at Ramakrishna Super Speciality Hospital for over 20 years, with laparoscopic mesh repair as the standard approach across all ventral hernia presentations.
Asymptomatic hernias that don’t meet surgical criteria are monitored with structured follow-up. When repair is indicated, a thorough pre-operative assessment determines the approach before any operative decision is made.
Midline upper abdominal pain or a small firm lump between the navel and breastbone?
FAQs
What is an epigastric hernia?
A protrusion of fat through a weakness in the linea alba, appearing as a firm midline bulge between the navel and breastbone.
Where does an epigastric hernia appear?
Midline upper abdomen, between the umbilicus and xiphoid process, along the linea alba.
Does an epigastric hernia always need surgery?
Small asymptomatic ones may be monitored. Symptomatic or enlarging hernias need laparoscopic mesh repair.
Can an epigastric hernia be repaired laparoscopically?
Yes. Laparoscopic mesh repair is the standard, with lower recurrence rates and faster recovery than open repair.
Disclaimer:
This blog is for educational and informational purposes only and should not be considered professional advice.