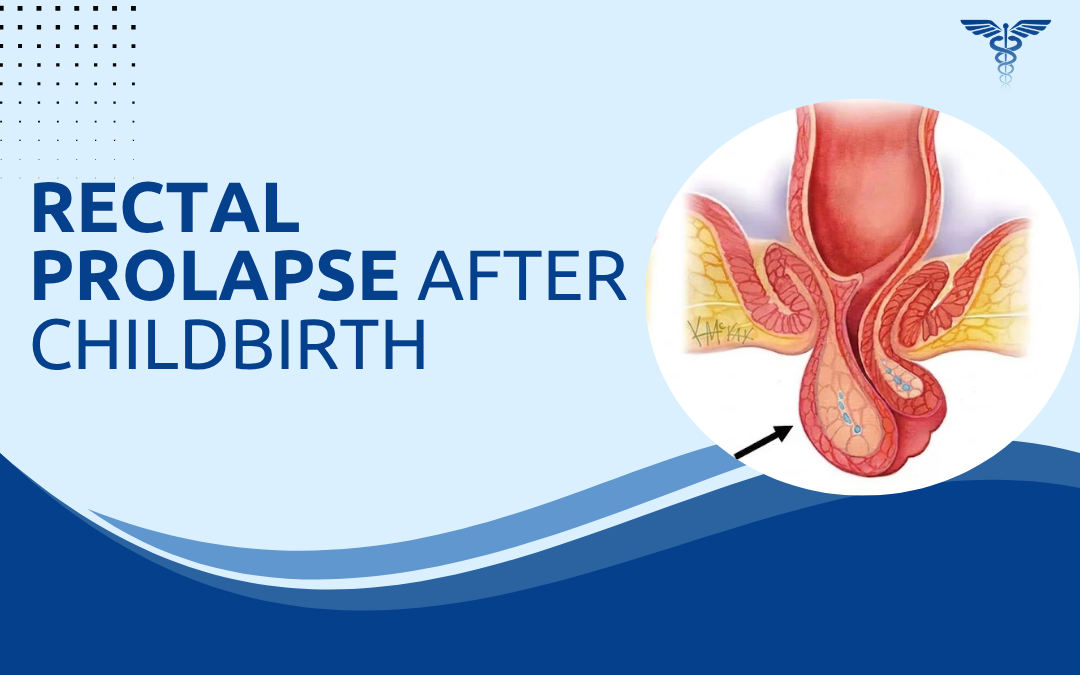
Rectal prolapse after childbirth is the full rectal wall sliding through the anus, not piles. Both protrude at the anus and both bleed, but the underlying structure is different. Prolonged second-stage labour, instrumental delivery, and multiple vaginal deliveries damage the pelvic floor support that holds the rectum in place. Once it fails, the rectum descends.
According to Dr. Rajeev Premnath, one of the best proctologist in Bangalore, “Postpartum rectal prolapse gets misdiagnosed as piles more often than most women realise. Both cause protrusion at the anus and both bleed. Without a proper examination, the wrong condition gets treated and the actual problem progresses untreated for months.”
How Does Childbirth Cause Rectal Prolapse?
Not every pelvic floor recovers fully from vaginal delivery. The structural damage can be subclinical for years before prolapse becomes apparent.
- Pudendal nerve damage: Prolonged second-stage labour or instrumental delivery stretches and partially denervates the pudendal nerve. Weakened musculature loses its ability to keep the rectum in position.
- Levator ani disruption: Tears, avulsions, and stretching during delivery create defects in the primary pelvic floor support layer. These don’t always heal completely.
- Multiple deliveries: Each delivery adds cumulative damage. The first may leave subclinical weakness. The second or third makes it clinical, sometimes years later.
- Instrumental delivery: Forceps and ventouse increase traction forces beyond spontaneous delivery. Pudendal nerve injury and levator avulsion are both more common as a result.
Postpartum rectal prolapse is frequently misattributed to piles in the months after delivery. A proper clinical assessment for piles treatment confirms which condition is actually present before any treatment decision is made.
How Is Postpartum Rectal Prolapse Recognised and Treated?
Diagnosis is clinical. An experienced surgeon can differentiate without imaging in most cases.
- Distinguishing from piles: Prolapse produces a circular red mass with concentric mucosal folds. Piles produce distinct separate cushions. The two look different. Treating one as the other wastes months.
- Symptoms beyond protrusion: Faecal incontinence, mucus discharge, and incomplete evacuation point to prolapse. Piles don’t cause incontinence. That symptom alone changes the diagnosis.
- Surgical repair: Laparoscopic rectopexy fixes the rectum to the sacrum with mesh or sutures. Perineal procedures are used when abdominal surgery isn’t appropriate.
- Timing: Most surgeons wait six to twelve months post-delivery before operating. Urgent repair is reserved for irreducible prolapse or mucosal ischaemia.
Rectal prolapse and piles need different management entirely. Our previous blog on postpartum piles covers how the two conditions present and how to tell them apart.
Why Choose Dr. Rajeev Premnath?
Dr. Rajeev Premnath is a General and Laparoscopic Surgeon with MBBS, MS (Gen Surg.), FRCS (Glasg.), FEBS, FICS, FACS, FIAGES, FMAS, and a Diploma in Laparoscopy from France. He’s been managing rectal prolapse and anorectal conditions at Ramakrishna Super Speciality Hospital for over 20 years, with laparoscopic rectopexy performed alongside the full range of proctological procedures across every presentation complexity.
Postpartum anorectal presentations here get properly examined before any diagnosis is confirmed. Prolapse doesn’t get treated as piles and piles don’t get sent for rectopexy.
Bulge or pain returning at an old hernia repair site?
FAQs
Can childbirth cause rectal prolapse in women?
Yes. Vaginal delivery damages pelvic floor support and the pudendal nerve, both of which keep the rectum in its normal position.
How is rectal prolapse different from postpartum piles?
Prolapse is the full rectal wall protruding. Piles are swollen anal veins. Different conditions, different appearance, different treatment.
Can rectal prolapse after childbirth heal on its own?
No. Pelvic floor exercises may reduce mild symptoms but full prolapse needs surgical repair.
How is postpartum rectal prolapse treated?
Laparoscopic rectopexy is the standard. Perineal procedures are used when abdominal surgery isn’t appropriate.
Disclaimer:
This blog is for educational and informational purposes only and should not be considered professional advice.